
Introduction
Intrauterine growth restriction (IUGR) defines a fetus that has experienced a decrease in his or her growth rate at some point during the pregnancy. This slow growth of the fetus is usually identified in utero with a series of ultrasound measurements that are followed over time. Many different factors can affect the growth of an embryo and then fetus. As such, there are many potential causes of this gestational growth restriction that can include environmental, maternal, placental and/or fetal problems.
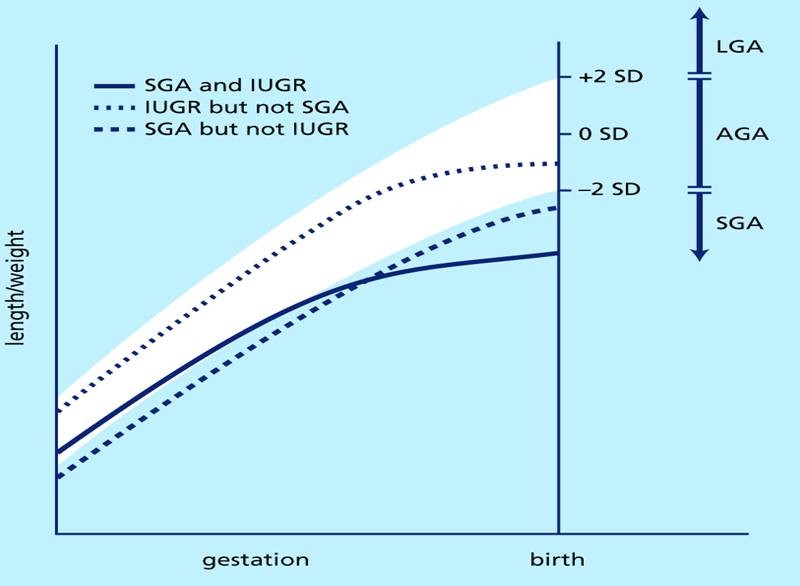
Because IUGR is a diagnosis based on growth during the prenatal timeframe, gestational age is an important determining factor. Gestational age is the amount of time that a fetus has spent in utero, and a routine average pregnancy is 40 weeks long dated from the first day of the mother’s last menstrual period. In order to determine whether a newborn has been born smaller than normal, gestational age has to be taken into account. There are different standards used to compare a newborn to other newborns – but in each, those newborns whose birth weight and/or length are between the 3rd and 97th percentile (adjusted for gestational age) are termed “appropriate for gestational age”, those whose birth weight and/or length are above the 97th percentile are termed “large for gestational age”, and those whose birth weight and/or length are below the 3rd percentile are termed “small for gestational age” (SGA).
A newborn may be born SGA, but not have evidence of IUGR if consistently small from the beginning of gestation. Conversely, a newborn who is large early in gestation who then experiences a period of IUGR may not be born SGA if his or her resultant size at birth is still greater than the 3rd percentile (approximately -2SDS on the chart below). In general, however, the majority of fetuses who are diagnosed with IUGR are also born SGA, but not all babies born SGA experienced IUGR.
The good news is that most IUGR/SGA babies experience immediate catch-up growth after birth, with the vast majority achieving full catch-up growth by age 2 years. In fact, if catch-up is to occur, it general occurs rapidly within the first 3 to 6 months after birth, and will typically be complete before 2 years of age. Premature IUGR/SGA babies may take longer to catch-up. However, research has found that about 10% of IUGR/SGA babies do not catch up in growth and remain small through adulthood, and these children can also face additional long-term health risks due to their intrauterine growth restriction.
Frequent Questions Parents May Ask
"How can doctors tell the difference physically between a baby who is small due to prematurity versus one who has experienced IUGR, if ultrasound evidence is not available?
Two criteria are used: physical (for example, skin texture and thickness, creases on the soles of the feet, firmness of ear lobes, and appearance of the genitals) and neurological (for example, posture or type of flexion of the hands and feet).
"Why is it important to determine whether a newborn is small due to prematurity or small due to IUGR?
The reason is that the potential medical difficulties after birth may be different. Some premature newborns have no problems at all whereas some may have immature lungs causing respiratory distress syndrome, "yellow" jaundice due to immaturity of liver function, and apnea which is an irregular breathing pattern caused by an immature nervous system. Infants born IUGR/SGA have an increased risk of meconium aspiration and thick blood (polycythemia). Many of the short-term issues of IUGR/SGA infants are similar to those seen in premature newborns, including hypoglycemia and hypocalcemia. Both groups of newborns must also be observed closely for signs of lack of oxygen, infection and low temperature (this latter problem in the IUGR/SGA infant results from the diminished fat tissue that normally helps maintain an infant's body temperature). Long-term health issues in former IUGR/SGA infants include possible early puberty, cardiovascular disease, hypertension, obesity, and metabolic syndrome/type 2 diabetes (T2DM).
"When should a pediatric endocrinologist (a doctor who specializes in growth disorders) be consulted for an IUGR/SGA baby or child?"
An appropriate time to contact a pediatric endocrinologist is when your child is still an infant (one year of age or less) and not catching up to the lower part of the normal growth range for his/her age (for example, less than the 3rd to 5th percentile on a height and/or weight chart). In rare cases, if this baby or child has very tall parents (75th percentile or higher), a pediatric endocrinologist should still be contacted even if the baby/child’s length remains at/about the 5th percentile. When your child is older, the doctor may recommend specific medical therapy to try to enhance your child's growth.
Causes of Intrauterine Growth Restriction (IUGR)/Small for Gestational Age (SGA)
IUGR/SGA can be caused by one or more factors from three primary categories -- maternal, fetal, and environmental factors and influences.
Maternal factors can include:
-
small size of the mother
-
mother's nutritional status during pregnancy
-
abnormalities of the blood supply to the placenta
-
abnormal shape or size of the mother's womb
-
diseases or conditions in the mother affecting her blood vessels such as high blood pressure, toxemia or eclampsia, recurrent bleeding during the pregnancy and diabetes mellitus
-
any chronic or prolonged illness in the mother such as diseases of blood cells (e.g., sickle cell anemia)
Fetal influences and factors can include:
-
chromosomal abnormalities or epigenetic errors resulting in any number of syndromes known to cause small size in the newborn
-
various fetal defects, including abnormalities of the heart
Environmental (outside and inside the uterus) factors can include:
-
defects related to the placenta and umbilical cord resulting in decreased oxygen and/or nutrients to the fetus
-
living at a high altitude
-
maternal smoking or drug use
-
population famine
-
multiple fetuses in the same pregnancy
-
maternal infection that crosses the placenta to the fetus
Outcome or Prognosis (Expectation in the Future)
The identification of IUGR prenatally and/or SGA at birth) is crucial because proper management can result in a better prognosis. In the newborn period, the doctors may want to do diagnostic studies to try and determine the cause of IUGR/SGA. They may also try to confirm the accuracy of the newborn’s gestational age. If the due date of a fetus was moved later during the pregnancy based on smaller-than-expected size, and the mother is confident of either her last menstrual cycle or date of conception, then the due date and gestational age should be readjusted based on this first calculation. [This results in a newborn being born closer to full-term than the adjusted due date and often results in a newborn now being diagnosed “small-for-gestational-age”.]
Ultimately, some of the most important aspects of IUGR/SGA are the intellectual or other neuro- developmental outcomes, including potential learning disabilities. These, to a major degree, reflect the underlying cause of the IUGR/SGA and highlight the importance of attempting to find out the cause(s) so that the appropriate plan of therapy is developed for the specific child. IUGR/SGA infants who are also born premature are at greater risk for medical problems than are full-term IUGR/SGA infants. But all children who experienced IUGR and/or were born SGA are at an increased risk for certain health issues in adulthood related to metabolic syndrome, including type 2 diabetes. And, for those who also fail to catch up in height, it is especially important that the child be referred to a pediatric endocrinologist experienced in treating growth failure (and the unique bone age advancement) of IUGR/SGA children.
Please refer to the MAGIC website information on children born small-for-gestational-age for more comprehensive information.
Important Steps for Parents
1) Prevention when possible (e.g., no smoking during pregnancy).
2) When IUGR is suspected, ensure that the pregnancy is monitored under the guidance of the obstetrician or physician specializing in high-risk pregnancies. Regular ultrasounds should be performed to monitor the growth restriction and assess for any other problems in the pregnancy.
3) When IUGR is identified and confirmed, appropriate treatment of the mother and fetus (and later, the newborn) should be implemented. Studies to determine the cause are quite important.
4) Parents, physicians and health-care workers need to combine forces to provide for the best possible outcome for the individual infant.
5) If the IUGR/SGA infant does not catch-up in length and remains either below the 3rd percentile, or more than 2 standard deviations below where the child should be for his/her parents (approximately fifty percentile points), the child should be referred to a pediatric endocrinologist familiar with treating IUGR/SGA children. The endocrinologist should also be familiar with the unique bone age advancement of these children.
6) Lastly, the child’s psychosocial and motor development should be assessed and monitored. All states have developmental evaluation and intervention services for children younger than age 3 years. These programs are based on the child's needs and not on parental income. For children over 3 years old, the school district becomes responsible for providing these services. Take advantage of this; intervention can make a world of difference for your child!
Written by:
Jennifer Salem, M.A.,
The MAGIC Foundation
RSS/SGA Research & Education Fund
&
Mitchell E. Geffner, MD
Professor of Pediatrics
Keck School of Medicine of USC
Chief, Center for Endocrinology, Diabetes & Metabolism
Children’s Hospital Los Angeles (CHLA)
Ron Burkle Chair in the Center for Endocrinology, Diabetes & Metabolism
Resources
» Download a printable version of the IUGR brochure
» Download a printable version of the Dental Problems Associated with Growth Hormone Deficiency brochure
» Download a printable version of the Psychosocial Impact of Short Stature on Children and Adolescents
» Download a printable version of the Frequently Asked Questions when Beginning Growth Hormone Therapy brochure
» Click here for member benefits or to join The MAGIC Foundation
» "LIKE" The MAGIC Foundation's Facebook page
» Would you like to speak to someone about IUGR? If so, call The MAGIC Foundation at 800-3MAGIC3 or (630) 836-8200 or Email Us
For assistance outside North America, visit our International Coalition to see resources in your country